This project seeks to examine and explore how the way we define geographical and occupational positions comes from an inherently racist set of principles
This project seeks to deconstruct the false perception a homogenous Latin American culture
This project exists to examine healthcare systems in the Americas and our attitudes toward them.
The project seeks to examine the culture impact of US imperialism in the 1900s on modern Latin American health system
This project seeks to explore how false perceptions of health in the Americas are harmful to all
This project seeks to have readers question their own personal biases surrounding race and health care
This project seeks to address the racist origins of American perspectives on global health
This project centers accessibility of knowledge and interaction with knowledge.
Why I am doing it
This project is my final assignment for my Core III class Landscapes of Plunder at Scripps College. Throughout the class we examined physical and societal landscapes and the origins of them. I initially set out to do this project because I was curious about why American think there are no doctors in Latin America, especially because I have friends who are currently studying medicine in Mexico and other places. I put out a survey to understand people’s varying perspectives on health in Latin America, and the responses generally showed the belief that the US has better health care than Latin America with many people rightfully noting that Latin America is a large area and that kind of comparison doesn’t really work. If you would like to see the survey responses for yourself, here are the US responses, and here are all of the responses. After doing some researched I recognized there were parts of Latin America that had really good health resources (Cuba) but weren’t presented as such and parts that didn’t. I wanted to examine what role, if any, imperialism had in creating these disparities. I also wanted to examine how our understanding of public health comes from bias. Through this project, I learned a lot about health care resources. While this is not comprehensive, I do believe that this is a good and accessible starting point for people who are trying to learn about public health as a product of colonialist plunder in Latin America.
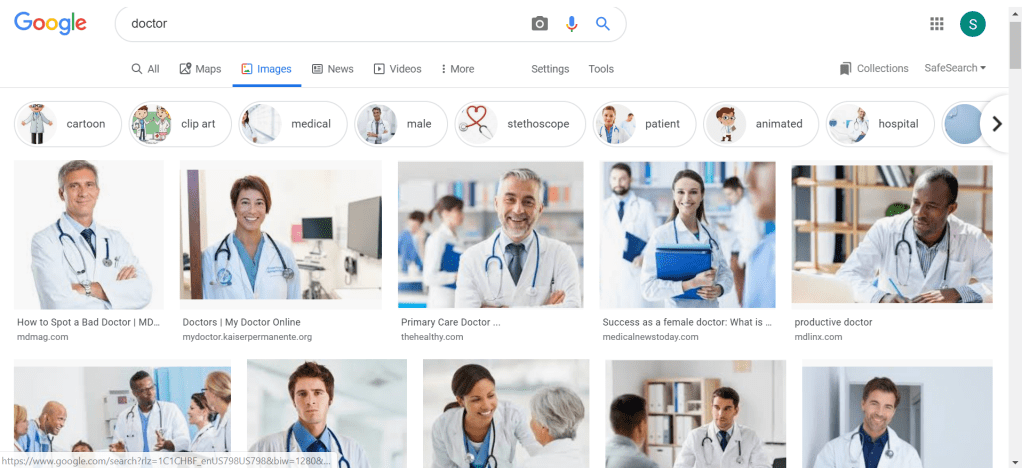
What do you think a doctor looks like? Here is what google thinks:
Image Description: google image results for the search term doctor
You’ll notice something about these images. Every single person wears a white coat, a stethoscope, most wear a smile. The majority are men, white men. And in the US, this is pretty similar to the statics we have: 69.8% of doctors are white, 61.6% of doctors are men and honestly, that sucks. (1)
But let’s look at a broader picture of medicine. The US is not the only place in the world with doctors, right? After all, article 25 of the UN declaration of human writes states:
“Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services.”
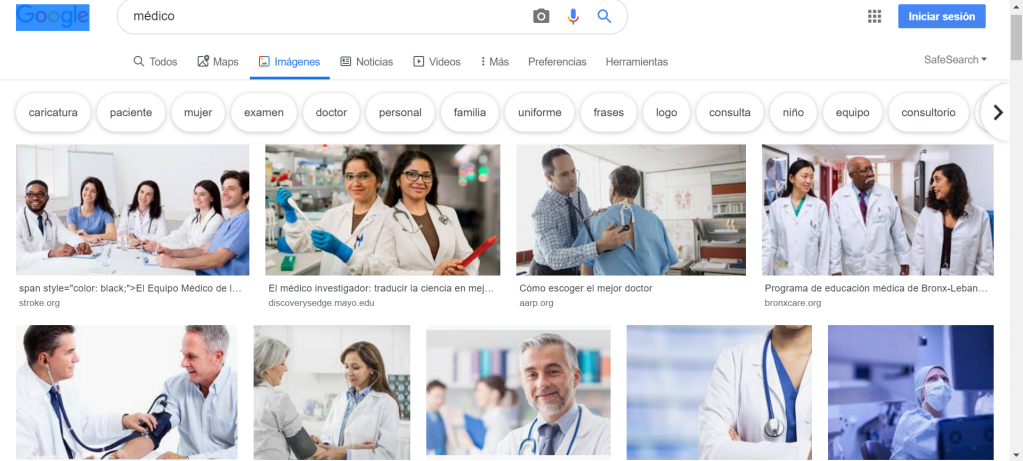
So what do we think doctors look like in other countries. First, I decided to ask what google images thought. I went to google.com.mx , searched medico and looked at the image results. (I recognize this isn’t peak investigative journalism, but I do believe it served its purpose)
Image Description: google.mx image results for the search term medico
Similarly, we see white coats, fake smiles, and stethoscopes. And interestingly enough, when you click on the links, they are Spanish web results for mostly american companies. Still, something has changed. In the top right image, you can see it’s an add for a medical service in the Bronx, but there are now doctors of color. It is reassuring to know there are resources in the United States for Spanish speaking populations, especially in areas such as the Bronx, which is over 53% Hispanic. However, it is stressful that Latin@ doctors only tend to pop up when you search in Spanish. Moreover, if I’m on google mexico, where are the doctors in Mexico? Who are they? What do they look like? And how do I find them?
The answer took me to some dark zones of internet statistics and even darker zones of health economics books (yikes!), and finally brought me back to the question, what even makes a doctor a doctor?
The answer to this question is different around the globe. So different, in fact that someone can be working in a country practicing medicine for years, only to move to another country and have to basically redo their degrees. This highlights a dangerous double standard in the medical industry. While doctors from other countries struggle have their degrees accepted, doctors with United States degrees can practice in other countries with relative ease. One US doctor remarked about his experience practicing in New Zealand:
The agency “just made everything so easy. They took care of all of the credentialing, visas, and passports. All [he] had to do was show up at the airport. Even [his] rental car was waiting for [him] at the airport when [he] got to New Zealand.”
At the same time, humanitarian International Non-Governmental Organizations (INGO) like Doctors Without Boarders (MSF) send doctors with foreign degrees to provide aide in times of need. While humanitarian aide can be beneficial, reliance on foreign aide can destabilize the startup of an industry in a “developing place.” Unlike medical missionary organisation which often function in order to provide care and converstion, MSF states in their charter: “Members undertake to respect their professional code of ethics and to maintain complete independence from all political, economic, or religious powers.” Still, these doctors inherently are practicing dangerous imperialist behavior, which range from working directly with the CIA to providing temporary care without any long term logistical planning, thus creating a damaging dependence. (For a deeper analysis on the imperialist powers of INGOs, check out this article.)
The imperialist nature of health science is not a new thing. There is a long history of healthcare being used as an imperialist practice. There are many ways this plays out. One important way is that advances in a nation’s health and sanitation practices and the implementation of these allows allows the nation to conquer a previously unconquerable area. A clear example of this is shown below.
In his 1913 book, The Triumph of American Medicine in the Construction of the Panama Canal, author J. Ewing Mears praises the health and sanitation practices of American doctors for creating a conquerable space in Panama, but you probably already guessed that from the title. In this book, Mears praises US sanitation and heavily implies that without it, the conquering of Panama would not have been possible (42). He claims that before US health advancements, Panama “has been known to be one of the unhealthiest regions of the Globe,” and it was “uninhabitable to any but the few natives who made their homes there, and the residents of the cities of Panama and Chagres,” due to malaria and yellow fever(26). I would question if Mears knows the definition of uninhabitable, as it is “(of a place) unsuitable for living in,” and it seems to me that by his own account, there were in fact many people living there. But I digress. Mears goes on to say that the purchase of Panama gave the US “sovereignty in that portion of the American Continent between Central and South America” and is as important as Jefferson’s Louisiana Purchase (20). This was true as it allowed America to become an economic and military powerhouse, as it provided a quick connection from the Atlantic to the Pacific ocean in a time that airplanes didn’t exist. Additionally, it gave the control needed for many later imperialist actions in Latin America. Finally, it allowed the US to see itself as a selfless benefactor to the people of Panama (check out this article for more information). This attitude of “selfless” violence can be summed up by the Monroe Doctrine, which I will write about later.
To get back to my initial question… What do you think a doctor looks like? If your answer looked something like the google image results, you too have been effected by the colonialist perspective of what health must look like. In our society, a doctor is a biomedical practioner and I doubt that will change for a while.
Still, there are systems that are looking to push the envelope on what medicine is and push back against imperialist sanitation forces.
Thank you for reading and let me know what you think in the comments.
It is hard to define Latin America because it is an inherently damaging definition. It defines a large region full of many countries and 2 continents as a product of their colonizers. Latin America refers to the formerly Spanish and Portuguese areas of the Americas. Often the term as used interchangeably with South America, but that is just wrong, as it excludes Mexico (a historically Spanish colony) and includes Guyana (an English speaking country that never really had anything to do with Spain.)
This gets kind of complicated when looking at parts of the US (read the American Southwest) which were formerly Spanish and still have a big Latin American presence and a lot of cultural ties and physical reminders of the former colonization. (A good book to read about this is Pasadena Before the Roses, which examines the cultural changes that Southern California went through in its early period.)
The false association of Latin America with South America allows Anglo-American nations (the US and Canada) to distance themselves from their continental neighbors. There are technically 23 distinct countries in North America, each with their own unique culture. Many are small Caribbean island nations and most of Central America is actually just North America, but when you ask most people what North America is, they say Canada, the US, and maybe Mexico.
In my research I found a dramatic example of this on a forum post for the popular video game, League of Legends. On this forum, entitled, “List of Countries that are in North America (and languages),” user MadLock attempted to clarify the players that were allowed to use the North American Server, that is the form of the game that was designed for north American players, and why English might not be the only language spoken on the server. MadLock lays out countries and languages spoken within them (14 are English speaking, 9 are Spanish speaking, and 4 speak French or another language.)
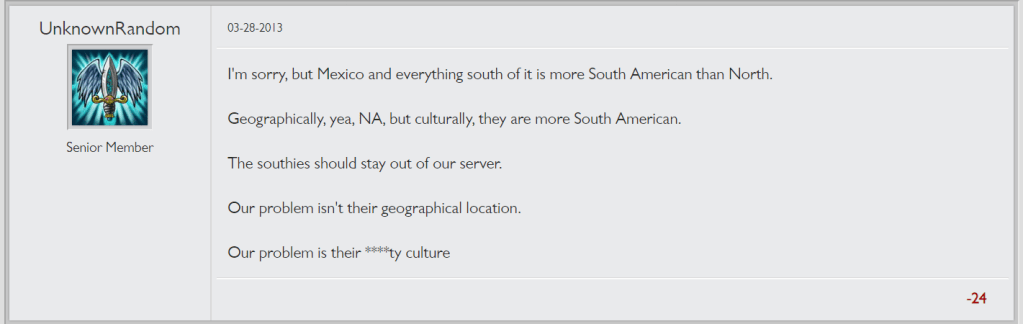
Another player disagreed with Madlock on this definition and gave his own opinion of what truly belongs in North America:
Image Description: a forum post by user “UnknownRandom” that states: “I’m sorry, but Mexico and everything south of it is more South American than North. Geographically, yea, NA, but culturally, they are more South American. The southies should stay out of our server. Our problem isn’t their geographical location. Our problem is their ****ty culture”
So yeah, if this doesn’t sum up Anglo-American white supremacy, I really don’t know what does.
As I said before, Latin America typically refers to formerly Spanish and Portuguese areas of the Americas, and for the purpose of this project, I will be using it as such. So that basically means (most of) South America, Central America, half of the Caribbean, and Mexico. Obviously, there is a lot of cultural variation in these places, but they tend to share language and (arguably) some elements of culture that combines indigenous, Spanish, and African practices. This is obviously a gross oversimplification of the cultural systems, but for the purposes of this project, we will be using the standard definition of Latin America.
Why look at Latin America as a system?
There is obviously a lot of differences in Latin American cultures, but when looking at Latin America through a medical and economic lens, that is a lens of resources, it is important to consider the history of colonization and the exploitation of resources that came out of that. The role of the Spanish colonies was to fund Spain. As a result of that Spain (and other colonizers) came in quick and bled the land and the people dry, terraforming and stripping the land of it’s richness both in soil and metal quality and forcing the indigenous populations into slavery.
After European coloniziers were removed, there were not that many resources left. Still, the resources that remained, such as the forests and oil reserves are owned and outsources by United States governmental forces. Through this, the United States has control over many valuable resources and economies. This allows the US to excercize negative influence on Latin American nations, and spread the idea of innate scarcity. There is not an innate scarcity of resources in Latin America. The financial and resoursal problems were purposely caused by the United States. Spreading the idea of innate scarcity allows the United States to appear blame free in the racist wealth gathering conquest that it continues to undertake.
Thus, we must look at Latin America as a system as it has been systamatically destroyed and defamed. We must keep in mind, however, that the differences in different areas are also important and making broad generalizations about Latin America feeds into the false stereotypes that the United States government wants us to believe.
The basis for my above opinions comes from Eduardo Galeano’s Open Veins of Latin America. This book provides a so called “peoples history” of Latin America. I suggest that everyone should read this book, as it is one of the reasons I began to investigate health care in Latin America.
There are a lot of common global markers of health that are used to define what countries are healthy and what health is. Today, I will split them up into two basic categories: determinant markers and outcome markers (a full list of WHO health indicators can be found here). Heath outcome markers deal with anything we can see as an outcome of “good” or “bad” healthcare. Some common examples of these are life expectancy, child mortality rates, and rates of illness. Determinant markers explore things like government spending on health, availability of healthcare, and vaccination efforts. (To learn more about why these are considered good markers of health, check out this link!)
Doctors per/population is often used as a marker of health as it is easy to visualize, and generally one of the easiest markers to visualize. It is important to think what makes someone a doctor before going into this, so hopefully you’ve read my post on that!
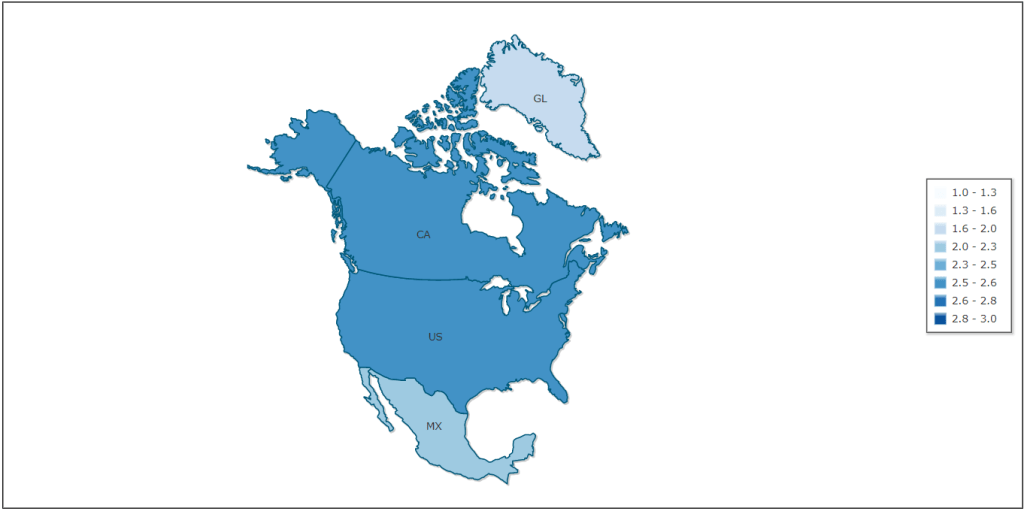
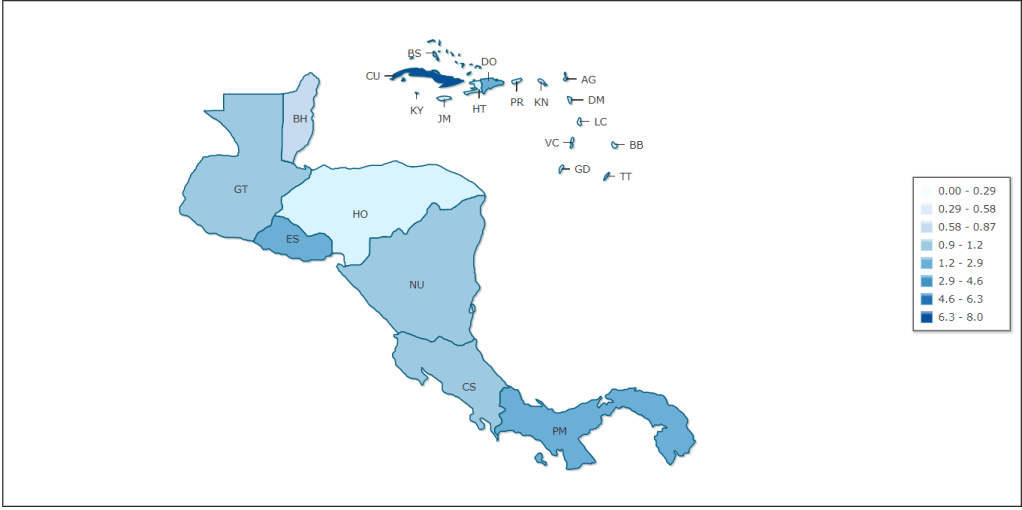
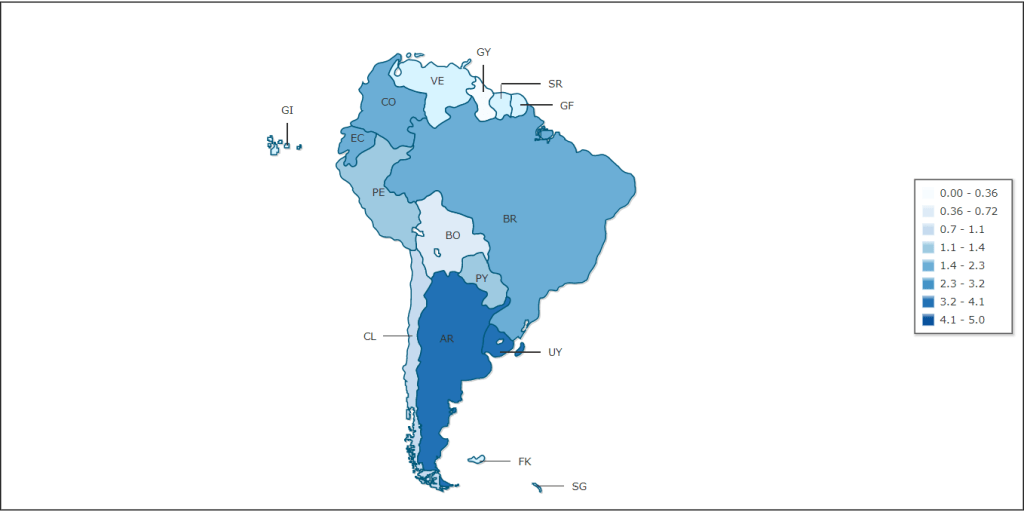
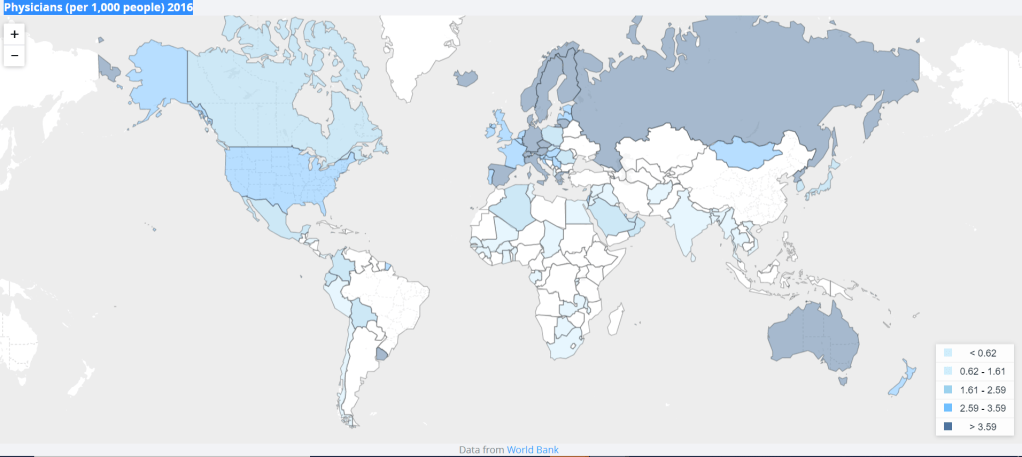
So what does doctors/1,000 look like globally? (Click this link for an interactive map as well other marker maps.) In 2016, it looked like this:
Image Description: Map of Physicians/ 1,000 in North America
Image Description: Map of Physicians/ 1,000 in Central America
Image Description: Map of Physicians/ 1,000 in South America
Image Description: a map of physician density per 1,000 people in 2016 Note, white areas are areas without data. The interactive map has a more comprehensive image.
On this map, it is difficult to see a lot of information, so I’d suggest taking sometime to check out the interactive version and looking over the last 10 years, as it gives a better picture of what physician density looks like as well looking at the interactive versions of the IndexMundi maps of North, Central, and South America.
Generally, health coverage in Canada and the US looks better compared to all of Latin America. This is a problematic generalization, as it does not show the full picture of care. Plus, because some of the countries in Latin America are so small that they are barely visible on the map. It is easy to assume, especially in larger countries, that the average number of doctors per 1,000 people gives a picture of health, but we must ask ourselves, is the distribution equal, and do more doctors really equal better health care.
In George Baziller’s 1960 critique of the American healthcare system, It’s cheaper to die, he claims that while in 1960, there were more doctors than ever before, the family doctor has become less available due to hyper-specialization. Furthermore, although there are enough doctors in the US, there aren’t the right kinds. You may be saying to yourself, but that book is old, surely things have changed. However, despite having one of the highest doctors per 1,000 in the Americas, the US still faces an upcoming healthcare shortage due to physician burnout and an aging population among other things. Additionally, in rural areas of the US, there simply is less access to healthcare. Is it possible that the shortage of doctors in Latin America is simply one of rurality? The short answer, no. The long answer… you guessed it… Imperialist practices. I digress.
I thought a good way to see if doctors really increased health was look at the relativistic lifespans of each place. So I did… and the data pretty much matches up. In places with more doctors/1,000 people on average tend to live longer. (If you’d like to see those maps for yourself click here, here, and here.) However, this is a very (very) loose correlation, as it’s not super proportional, nor is it always true that more physicians bring about better health.
I began to research other forms of medical practitioners. It is fairly easy to access information about physicians, but it is much harder to find information on total health professionals, that is midwives, ethnomedical practitioners, nurses, nurse practitioners, etc. Within this I allowed myself to wonder why the solution to scarcity of doctors by the United States often seems to be sending foreign medical practitioners rather than building up systems of education.
All of this led to a scary truth. The healthcare crisis in Latin America has been purposely manufactured. The way we measure health systems, as well as how they are formed has been manufactured along side this to exploit various places for their resources around the globe. I will further discuss the imperialist practices present in determining health as well as how health creates paths for violent imperialism.
Thanks for reading. Please comment with your own thoughts
Biomedicine is what we think of as “modern” medicine or “western” medicine. It is sanitation, vaccination, antibiotics, the type of medicine based on disease and microbiology. To call biomedine “modern” and “western” is a lie, as disease prevention is an ancient as aqueducts, and understanding of illness extends much beyond the western world (Bastien-x, Porter-2).
Ethnomedicine is what we think of as “traditional” or “regional” medicine. It is the medicine based on folk lore, herbology, experience, and understanding of a patient’s health as not just the mind’s relationship with the body, but the bodymind’s relationship with the universe. Ethnomedicine takes different forms in different places. It is a place and people specific ideology surrounding health (Bastien- x-xi)
There is an emphasis in contemporary academic circles on biomedicine over ethnomedine. Often, biomedicine is curative, that is it isn’t used until someone gets sick. It is therefore easy to prove that it works because if people recover or have a decrease in symptoms, it can be connected to the medicine through clinical trials. Ethnomedicine is often more preventative, which is harder to prove if something works. For example, if you take something and you don’t get sick, how do you know you weren’t going to get sick in the first place. In our society, biomedicine has thus been deemed more useful. Biomedicine also works with the capitalist systems of insurance and pharmaceuticals that much of the world has.
Let me know what you thing about ethnomedicine in the comments! Should we try integrating it and making our medical system all around more holistic?
In 1823, James Monroe told European nations that they had no right to interfere in the Western Hemisphere. The US wanted the European colonizers and shadow governments out. And conceptually that sounds like a good thing, except the problem was the US government wanted to replace those shadow governments with their own.
Throughout the 19th and 20th centuries, the US then used this policy to gain control as the policing force for the Western Hemisphere. In 1904, President Theodore Rosevelt stated that it was an “international power police,” and pretty much acted like that until today.
And with this power, has the US government spread peace, love, and democracy. The answer is no. Through this policy, the US has been responsible for many military coups and shadow governments throughout the Americas. (https://www.ourdocuments.gov/doc.php?flash=false&doc=23#)
Below is a short video that outlines just some of the damage that these interventionist policies have had, specifically in how they effected the current crisis in Venezuela.
A video dealing with US interventionist policies and the current economic crisis is Venezuela
If you would like to learn more about the practices associated with the Monroe Doctrine in general, this timeline from North Carolina State University and this KCET timeline are a good place to start. To learn more about how these practices have affected health care in Bolivia, Venezuela, and Cuba, go to the next post!
Latin America has a history of successful implementation of socialized health. The movement for socialized health came up in the 1950s and 60s. The Latin American Social Medicine is organized around the Latin American Association of Social Medicine (founded 1984). To learn more about the history of this movement, check out this article. Latin Americas history of socialism has made it a target for US imperialist programs and rhetoric. Here are some examples the ways in which socialized medicine is carried out in Latin America and the ways that the US has tried to interfere.
Cuba: A model for socialized health care in Latin America
Across the board of health care markers, Cuba’s resources rank similar or better than the US. Still, there are posts angled at Americans on how to provide aid to Cuba. Part of this comes from the idea that Cuba is facing an economic crisis and does not have enough money to provide for its people. This isn’t true. In Steve Brouwer’s Revolutionary Doctors: How Venezuela and Cuba are Changing the World’s Conception of Health Care, he discusses the long history of the Cuban economy, and how that has effected the way the Cuban health care system exists today.
What it comes down to is a war of ideas. Cuba chose to put quality of life above traditional markers of capitalist success. And for that it has been punished. The US has actively spread hateful rhetoric about these health care systems in order to defame Cuba. In 2006, Michale Parmly, head of US Interest Section in Havana sent out a cable to Latin American embassies asking for “human interest stories and other new that shatters the myth of Cuban medical prowess.” (Browner 211). The United States has further targeted Cuban medical systems, going so far as to hide that Cuba provided the greatest medical aide after the Haitian earthquakes (213).
Cuba has used its extensive medical system to provide care not only in Cuba but in other areas of Latin America. Through these next sections, you will see how Cuba has led health care changes across Latin American, and why its systems are deemed such a threat.
In 2000, shortly after becoming president of Venezuela Hugo Chavez began to make deals with Cuba regarding changes in health care and education. This was made possible by the construction of new systems of education. In 2002, a US backed coup against Chavez occured, but he remained in power (Brouwer 182), for more information about that coup, read this article.
Bolivia: Can it overcome a history of medical imperialism?
Bolivia and Haiti are considered to be the countries in the Americas that consistently rank the worst across all health care markers (link for post). I want to examine the history of why Bolivia has such low health care numbers. First, Bolivia’s geography makes it difficult to provide care to every area as the types of diseases present have much variability. This theoretically could help explain why Bolivia seems to have particularly bad health. But this is not the only factor.
Bolivia, like many places in Latin America has had difficultly keeping a stable government. Here is a short video about the history of the nation. This video does not give a full picture of Bolivia’s history, nor does it discuss the practices of indigenous Bolivias with a great deal of respect. However, it is short and I believe it will give us enough of a starting ground to talk about Bolivia’s healthcare.
From this video, we can see that many of Bolivia’s resources such as the silver from the Cerro Rico were stolen. In its first hundred years as an independent nation, it lost a lot of its territory to Chile (which often has accepted US aid) and Brazil. During this time period, healthcare was unstable do to wars and disease outbreaks. In Ann Zualaski’s book Unequal Cures, she outlines some of the disparities in the Bolivian health care system from 1900-1950. From 1932 to the first revolution in 1952, the Rockefeller foundation (Yes, the same Rockefellers as Rockefeller Standard Oil) came to Bolivia to provide health care as well as “promote U.S. economic and political interests through the eradication of epidemic diseases and the development of U.S. style medical institutions” (Zulawaski 87). Effectively they used the promise of medical help as a form of societal control. Like the canal zone in Panama (see this post), a main goal was strict sanitation measures to rid the country of yellow fever. Hidden in this was a desire for free Bolivian oil, as the Yellow Fever Service from RF was allowed to use Bolivian oil for free. Throughout the 1940s, the US government, as well as UNICEF and the WHO began offering alternatives to the Rockefeller Foundation. As a result of this, the foundation began to change their model away from the focus on yellow fever and towards a more holistic approach for the Latin America, including the training of doctors. Bolivia was left out of this, however, because it was thought to not have enough resources to support medical training programs. By the end of the 50s, they had mostly moved out of Bolivia claiming that “the country was too poor to benefit from its programs…and too backward scientifically to receive much support” from the medical training programs (115). The Rockafeller Foundation prevented a medical industry from forming in Bolivia with their invasionatory practices and refusal to implement education. Thus, by the early ’50s, the political climate in Bolivia was unstable and ripe for revolution.
From 1950s to the 1980s there were many military coups and unstable governments. It was during this time that US forces put down several uprisings with more leftist leanings, including murdering Che Guevara in 1967. They then further supported the rise to power of dictators such as Banzar. There then was a period of “democracy” in which strict economic policies from the US led to many Bolivians becoming or staying impoverished. In 2005 Evo Morales, an indigenous Bolivian was elected president. Morales made many changes to the health care systems of Bolivia, adding in elements of socialism. Beyond this, many important Bolivian resources were nationalized, such as gas and oil, pushing out many foreign companies (Read this article to learn about the the nationalization of oil in 2006) This year, Morales was forced to resign from presidency due to a military coup. Many pro-socialist groups claim that this Coup, like the right wing coups before it, had US backing. (x, x, x)
Under Morales, there were many changes to the healthcare system in Bolivia. One of the most important changes was the integration of ethnomedical practices into governmental health spending (x). To learn more about the roots of ethnomedical and biomedical integration, read Drum and Stethoscope. Additionally, Morales employed the Cuban “Yo, Si Puedo,” in order to help end illiteracy. Within 2 years the rate of illiteracy went from 13.28% to 3.8%, which means that under the UNESCO definition, Bolivia had eradicated illiteracy. Cuba supported Bolivia as well by sending over doctors and creating ALBA scholarships for Bolivian doctors to study in Cuba. (190). It is difficult to say what will happen in Bolivian health care do to the current change in governmental leadership.
Final thoughts
The patterns of US medical imperialism extend beyond Latin America. The roots in the oil industry and other capitalist gains are scary. The continuation of US backed coups as evidenced by Bolivia and Venezuela shows the United States is not willing to give up their power anytime soon.
I read a lot of books and articles for this project, so many in fact that all of them were not able to make it into my final work. For this page I am focusing on books that I truly believe would be a good place to start for understanding the history and continuation of medical imperialism, as well as different medical practices in Latin America. Some of these were referenced throughout this blog while others simply informed my perspectives. All of these books are available at the Honnold-Mudd library in Claremont California.
Open Veins of Latin America- Eduardo Galeano
Revolutionary Doctors: How Venezuela and Cuba and Changing the World’s Conception of Health Care- Steve Brouwer
Unequal Cures: Public Health and Political Change in Bolivia, 1900-1950- Ann Zulawski
Drum and Stethoscope: Integrating Ethnomedicine and Biomedine in Bolivia- Joseph W. Bastien
The Triumph of American Medicine in the Construction of the Panama Canal- J. Ewing Mears, M.D. LL. D
It’s Cheaper to Die: Doctors, Drugs, and the A.M.A- William Michelfelder
Science, Medicine & Cultural Imperialism- Edited by Teresa Meade and Mark Waker
Doctora in Mexico: The Life of Dr. Katherine Neel Dale- Olive Floyd
Cultural Differences and Medical Care: The Case of the Spanish-Speaking People of the Southwest- Lyle Saunders
Primary Health Care in Cuba: The Other Revolution- Linda M. Whiteford and Laurence G. Branch
Health, Civilization and the State: A History of Public Health from Ancient to Modern Times- Dorothy Porter
Hygienic and Climatic Conditions in the Leading Cities of Latin America (1939)- Compiled by N.A. Brown
Health and Health Care in Latin America During the Lost Decade: Insight for the 1990s- Connie Weil and Joseph L. Scarpaci
Pricing Life: Why It’s Time for Health Care Rationing- Peter A. Ubel, M.D.
Irrationality in Health Care: What Behavior Economics Reveals About What We Do and Why- Douglas E. Hough
Entre Medicos Y Cuaranderos: Cultura, Historia y Enfermedad en la America Latina Moderna- Diego Armus
The Health and Survivial of the Venezuelan Yanoama- Marcus Colchester
Thank you! Let me know if you have suggestions in the comments!